


SOMA.PRU
Biological and psychosocial factors affecting the persistence of pruritus symptoms
Background
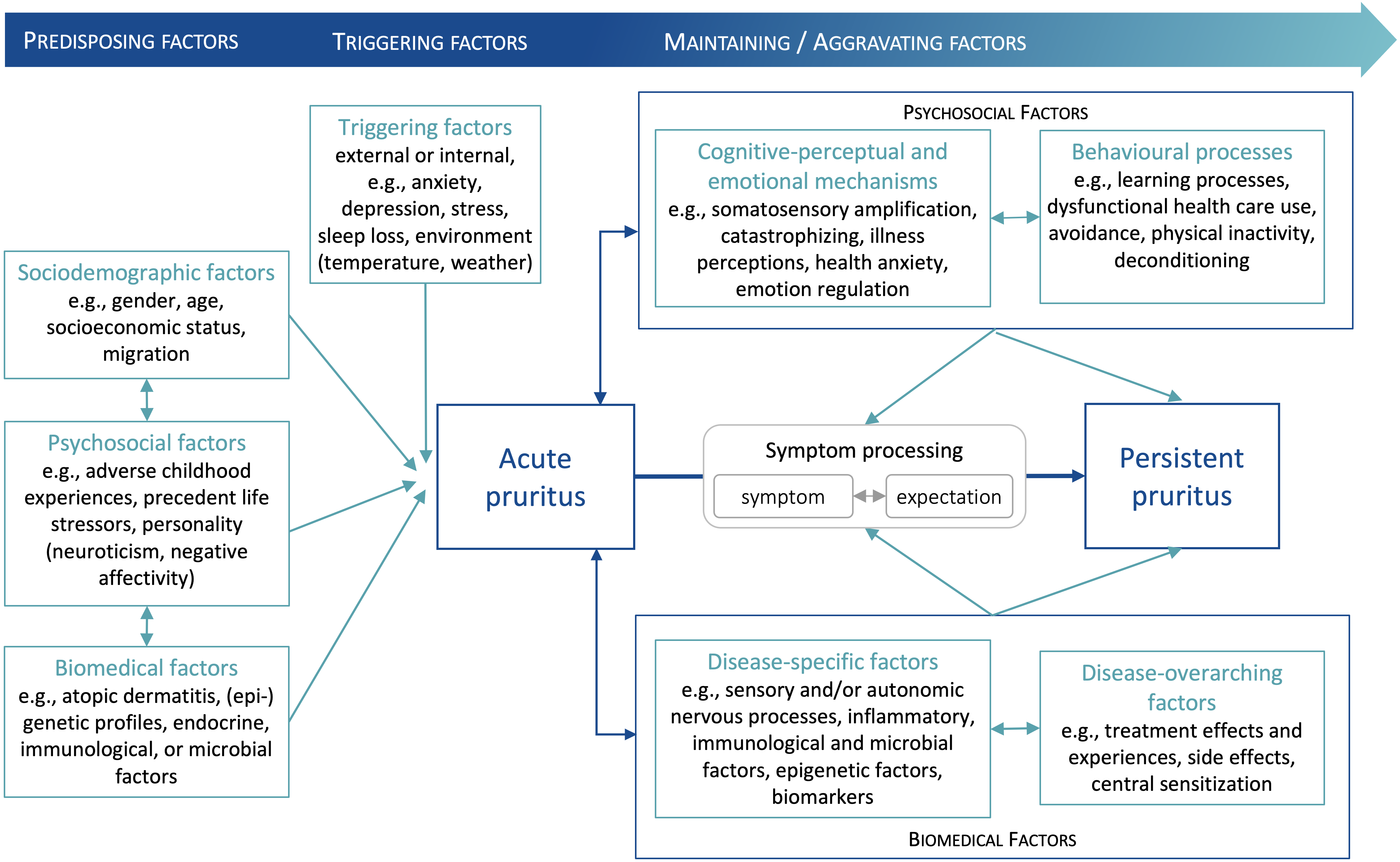
Chronic pruritus (CP), or persistent itching, is a symptom of many dermatologic, neurologic, systemic, and psychosomatic diseases. CP has a prevalence of ~20% in the general population and is therefore a significant burden on society, but the transition from acute pruritus to CP is not well understood and probably involves interactions between multiple biological, environmental and psychosocial factors. Acute pruritus is triggered by chemical, physical or mechanical stimuli, whereupon neuro-immune crosstalk is best understood and has the highest clinical relevance. The transition to CP is likely to involve pruritus-specific risk factors as well as mechanisms shared with other persistent somatic symptoms, which are addressed in other projects of the RU SOMACROSS programme.
Aims
We aim to identify psychosocial and biological factors, as well as their interactions, contributing to the persistence of CP with and without neuro-immune cutaneous crosstalk. In addition, we expect that psychosocial factors relevant to the persistence of symptoms in conditions such as fatigue and pain, including somatosensory amplification, illness anxiety, depression, stress, and symptom or treatment outcome expectations, may also contribute to CP.
Working programme
Three cohorts of patients with acute and chronic atopic dermatitis (immunologic background) and CP patients with unaffected skin (non-immunologic background) will be recruited for a comprehensive translational investigation. This will address pruritus-specific and all shared psychosocial assessments in the RU SOMACROSS programme, including neurological parameters (using quantitative sensory testing), cutaneous nerve fibre morphology, skin barrier morphology, epidermal metabolism, and pruritogen blood levels. Within one year, patients and matched healthy controls will be investigated at three time points, allowing the cross-sectional comparison of acute atopic dermatitis, chronic atopic dermatitis, CP on unaffected skin, and healthy controls, and a longitudinal investigation of predictive outcome factors in these patients under treatment according to existing guidelines.
Expected impact
We expect to identify pruritus-specific psychosocial and biological factors (including peripheral skin barrier effects and central neuronal sensitization processes), as well as mechanisms shared with other persistent somatic symptoms, which interact to promote the persistence of CP symptoms. These results will be transferred to the clinic to improve the treatment of CP and will allow the development of new hypotheses explaining the persistence of other chronic somatic symptoms.
-
Image information
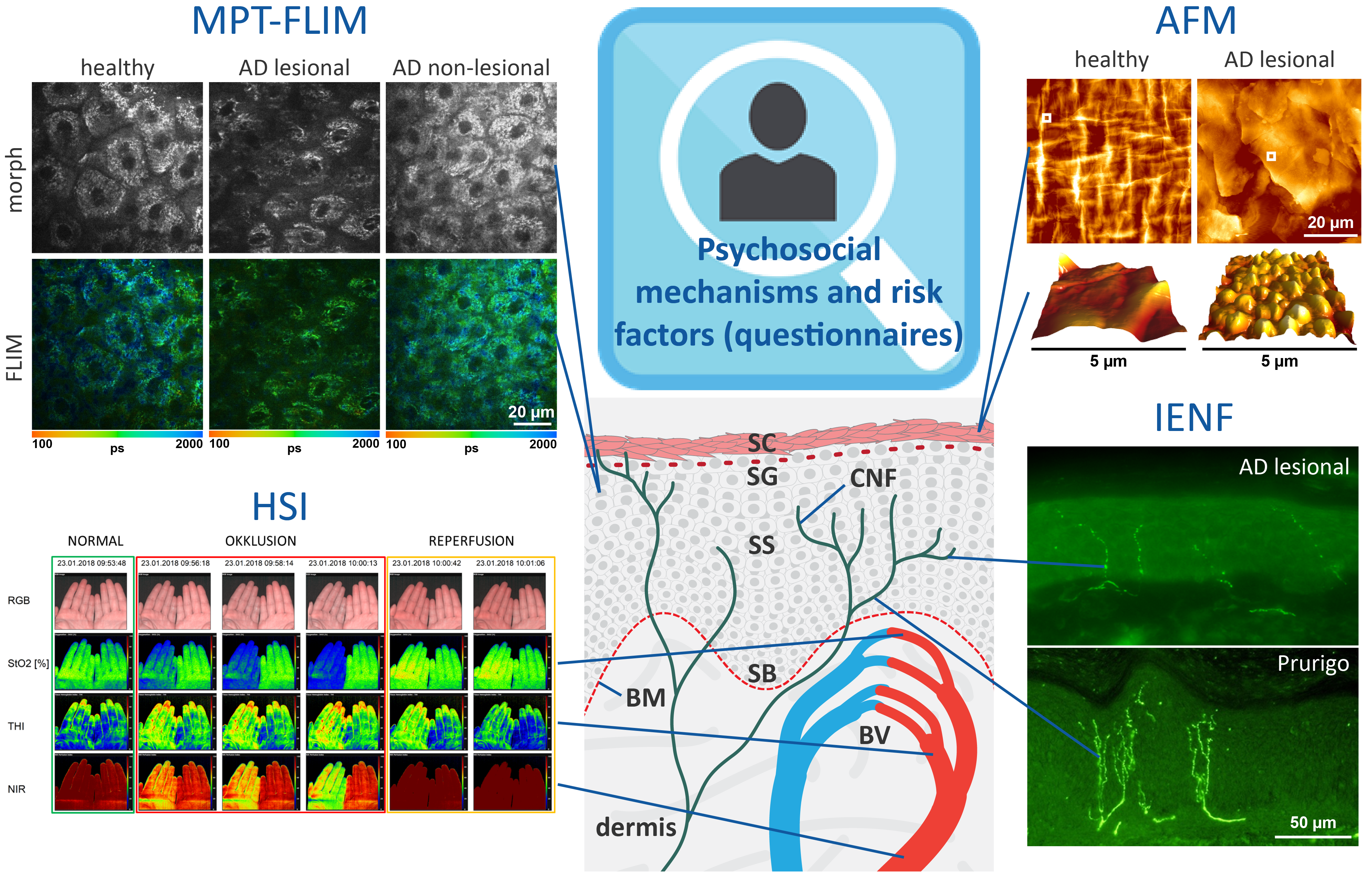
An overview of methods and questionnaires applied to correlate psychosocial factors, structural and pathophysiological dysfunctions as risk factors for chronic itching.
Schematic skin model: SC, stratum corneum (main skin barrier); SG, stratum granulosum, SS, stratum spinosum; SB, stratum basale; BM, basement membrane; BV, blood vessels; CNF, cutaneous nerve fibres.
Psychosocial predisposing, triggering and maintaining/aggravating factors, as well as some of the primary and secondary outcome measures, will be recorded using a comprehensive set of validated and reliable questionnaires and rating scales, which will be applied at each visit. These comprise the core set of questionnaires of the research unit, as well as pruritus-specific questionnaires. Pruritus-specific and generic predictors and outcome measures, including the questionnaires are summarised in table 1.By applying non-invasive multiphoton tomography equipped with a fluorescence lifetime imaging module (MPT-FLIM), high-resolution morphological imaging of distinct layers of the skin (morph) will be combined with fluorescence lifetime imaging-based single-cell metabolic characterisation (FLIM).
Furthermore, hyperspectral imaging (HSI) of the target skin area will facilitate the quantification of oxygenation levels (StO2 [%]), haemoglobin saturation of the tissue (THI) and peripheral blood perfusion (NIR). After tape stripping, atomic force microscopy (AFM) will allow the nanoscale quantification of individual corneocytes, intercellular gaps, corneodesmosomes and claudin-1 levels. PGP9.5 staining followed by fluorescence microscopy will allow the analysis and quantification of intraepidermal nerve fibres (IENFs).
Cutaneous neuroanatomy differs between CP patients and healthy controls but also between different CP entities (upper panel, atopic dermatitis, lower panel, prurigo nodularis). MPT-FLIM, HSI, AFM and IENF will be combined for the analysis of CP-related metabolic changes, disruption of skin barrier integrity and innervation of the skin as novel objective parameters representing the severity of CP. AD, atopic dermatitis; CP, chronic pruritus.


