Project - A08:
Spatial decoding of hepatic microenvironments to decipher, diagnose and stratify autoimmune hepatitis
Project leaders:
Prof. Dr. Victor Puelles, MD, PhD;
Prof. Dr. Marina Zimmermann &
PD Dr. med. Marical Sebode, PhD



Summary
Autoimmune hepatitis (AIH) is a severe liver disease with an unknown aetiology. Untreated AIH progresses to cirrhosis, liver insufficiency and death. AIH can manifest acutely with high hepatic inflammatory activity or asymptomatically with mild and chronic liver damage. Given the potential consequences of AIH, life-long immunosuppressive treatment is needed in the majority of patients. However, treatment of AIH is associated with severe side effects and limited quality of life. To date, the following aspects of AIH remain poorly defined:
A) Pathogenesis: The pathogenesis of AIH is incompletely understood. First, AIH can manifest from early childhood to old age. Importantly, the trigger for disease manifestation remains unknown. It has been proposed that environmental antigens such as viral infections or the intake of an immunogenic drug or food component could trigger an autoimmune reaction that results in AIH in genetically susceptible individuals. The inflammatory activity of AIH fluctuates between times of very strong inflammation, leading to a clinical flare and times of low or even no activity, allowing the weaning out of immunosuppressive treatment. Furthermore, some patients have a more aggressive disease course, since first-line treatment is not sufficient to achieve remission and these patients require second- or third-line treatment with more potent immunosuppressants. To decipher the mechanisms that define the chronic autoimmune reaction in AIH, the comparison with drug-induced liver injury (DILI) is helpful. The presentation of DILI resembles the acute manifestation of AIH without a chronic course. For the analysis of the chronic course of AIH, patients with chronic viral hepatitis B (HBV) and D (HDV) infection can serve as controls for an immune reaction directed against a persisting antigen. By comparing the hepatic microenvironment of AIH to other liver diseases that are defined by concrete triggers and clinical courses, we will have an opportunity to carefully dissect AIH pathogenesis, aiming to enhance patient care at multiple levels, including identification of novel therapies, monitoring tools, diagnosis and prognosis.
B) Diagnostic accuracy. The diagnosis of AIH is complex and mainly based on clinical scores, since specific diagnostic tests do not exist. A liver biopsy is mandatory but can be inconclusive as multiple conditions resemble AIH. As mentioned above, DILI is a key differential diagnosis for acute AIH and cannot be differentiated from acute AIH with certainty, even assessing liver histology. DILI can present as acute hepatitis, but in contrast to other acute liver diseases such as viral hepatitis, DILI lacks specific diagnostic tests, similarly to AIH. However, DILI is not a chronic disease and does not require long-term immunosuppressive treatment. For this reason, if DILI is misdiagnosed as AIH, patients will receive unnecessary long-term immunosuppression. Furthermore, if AIH is misdiagnosed as DILI, patients are at risk of a disease flare as they are not protected by immunosuppressive treatment. Therefore, avoiding misdiagnoses is highly relevant for patients with AIH or DILI. Another diagnostic uncertainty concerns variant syndromes, as AIH can further present with additional clinical features of primary biliary cholangitis (PBC), which is known as variant syndromes (VS), affecting about 10-20% of patients. AIH is characterised by inflammatory activity primarily directed against hepatocytes that can involve bile duct damage to some degree, whereas PBC is a cholestatic liver disease with progressive destruction of small intrahepatic bile ducts that can be accompanied by some degree of inflammatory activity beyond the bile ducts and portal tracts. While there is no international consensus on the pathogenesis and diagnosis of VS, this has direct therapeutic and prognostic implications, especially as it is unknown which patients will benefit from immunosuppressive treatment (targeting features of AIH) and which patients can be treated solely with ursodeoxycholic acid (targeting features of PBC).
C) Risk stratification. There is currently no test available to predict the response to the standard immunosuppressive treatment for AIH. Importantly, difficult-to-treat patients are at very high risk for disease progression and cirrhosis. Current treatment algorithms recommend achieving complete biochemical remission in AIH, which is defined as normalised transaminases and IgG after 6 to 12 months of treatment. If remission is not achieved, second- and third-line treatment will follow, again each taking several months until its success can be evaluated. During this time, the patient is under continuous risk of disease flares and progressive liver damage. It is an urgent clinical need to identify those patients who are at high risk of having such an aggressive clinical course to start with more potent immunosuppression in early stages of AIH.
In this context, we hypothesise that the histological area of the portal tract interface in patients with AIH contains critical mechanistic, disease-specific and prognostic spatial data. Thus, project A08 proposes to utilise our team’s expertise that combines novel microscopy-based molecular tissue profiling, medical experience and access to unique patient cohorts with extensive clinical phenotyping. We will use innovative computational image analysis tools to perform subcellular proteogenomic mapping of the hepatic microarchitecture typical of AIH, leading to a better understanding of the pathogenesis and the development of better tools for diagnosis and risk stratification of patients with AIH and also patients with DILI, HBV and HDV. The insights gained in project A08 will offer a deeper understanding of more general mechanisms of autoimmunity directed against the liver, which may serve as a resource for other projects in this CRC and as a hypothesis generator for future funding periods.
Project plan
Our central hypothesis is that the histological area of the portal tract interface in AIH patients contains critical pathogenetic, disease-specific and prognostic spatial data.
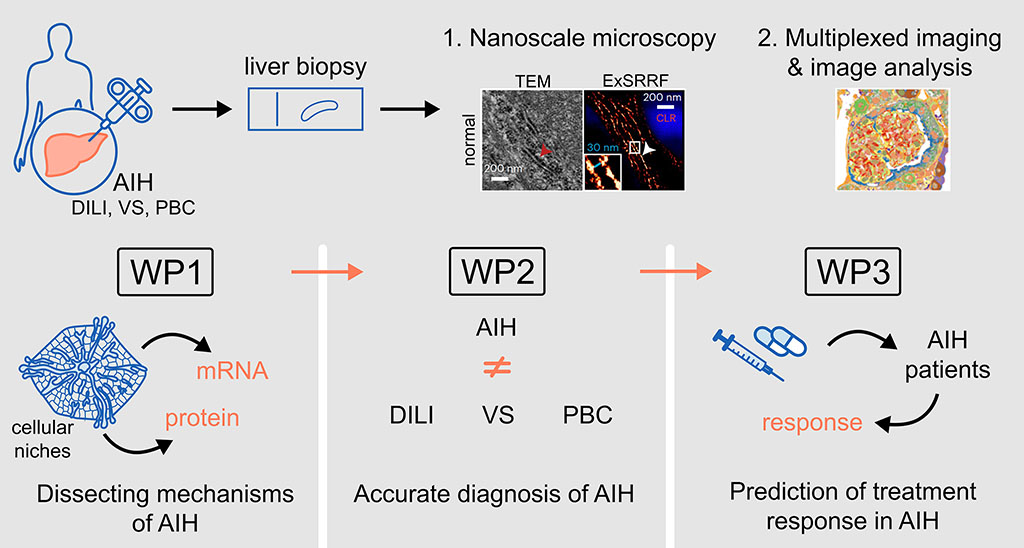
In order to test this hypothesis, our work programme has the following work packages (WP):
WP1: To dissect pathophysiological mechanisms of AIH.
WP2: To differentiate AIH from key differential diagnoses.
WP3: To predict the treatment response in patients with AIH.
Project related publications
Peiseler M, Sebode M, Franke B, Wortmann F, Schwinge D, Quaas A, Baron U, Olek S, Wiegard C, Lohse AW, Weiler-Normann C, Schramm C, Herkel J. FOXP3+ regulatory T cells in autoimmune hepatitis are fully functional and not reduced in frequency. J Hepatol 2012;57:125-32. doi: 10.1016/j.jhep.2012.02.029. Open Access.
Lohse AW#, Sebode M#, Bhathal PS, Clouston AD, Dienes HP, Jain D, Gouw ASH, Guindi M, Kakar S, Kleiner DE, Krech T, Lackner C, Longerich T, Saxena R, Terracciano L, Washington K, Weidemann S, Hübscher SG, Tiniakos D. Consensus recommendations for histological criteria of autoimmune hepatitis from the International AIH Pathology Group: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology. Liver Int 2022;42:1058-1069. doi: 10.1111/liv.15217. Epub 2022 Mar 12.
Marjot T#, Buescher G#, Sebode M#, Barnes E, Barritt AS 4th, Armstrong MJ, Baldelli L, Kennedy J, Mercer C, Ozga AK, Casar C, Schramm C; contributing Members and Collaborators of ERN RARE-LIVER/COVID-Hep/SECURE-Cirrhosis; Moon AM#, Webb GJ#, Lohse AW#. SARS-CoV-2 infection in patients with autoimmune hepatitis. J Hepatol 2021;74:1335-1343. doi: 10.1016/ j.jhep.2021.01.021. Open access.
Lohse AW, Sebode M, Jørgensen MH, Ytting H, Karlsen TH, Kelly D, Manns MP, Vesterhus M; European Reference Network on Hepatological Diseases (ERN RARE- LIVER); International Autoimmune Hepatitis Group (IAIHG). Second-line and third- line therapy for autoimmune hepatitis: A position statement from the European Reference Network on Hepatological Diseases and the International Autoimmune Hepatitis Group. J Hepatol 2020;73:1496-1506. doi: 10.1016/ j.jhep.2020.07.023.
Kylies D, Zimmermann M, Haas F, Schwerk M, Kuehl M, Brehler M, Czogalla J, Hernandez LC, Konczalla L, Okabayashi Y, Menzel J, Edenhofer I, Mezher S, Aypek H, Dumoulin B, Wu H, Hofmann S, Kretz O, Wanner N, Tomas NM, Krasemann S, Glatzel M, Kuppe C, Kramann R, Banjanin B, Schneider RK, Urbschat C, Arck P, Gagliani N, van Zandvoort M, Wiech T, Grahammer F, Sáez PJ, Wong MN, Bonn S, Huber TB, Puelles VG. Expansion-enhanced super-resolution radial fluctuations enable nanoscale molecular profiling of pathology specimens. Nat Nanotechnol 2023;18:336-342. doi: 10.1038/s41565-023-01328-z. Open access.
Zimmermann M#, Klaus M#, Wong MN, Thebille AK, Gernhold L, Kuppe C, Halder M, Kranz J, Wanner N, Braun F, Wulf S, Wiech T, Panzer U, Krebs CF, Hoxha E, Kramann R, Huber TB#, Bonn S#, Puelles VG#. Deep learning-based molecular morphometrics for kidney biopsies. JCI Insight 2021;6:e144779. doi: 10.1172/jci.insight.144779. Open access.
Ragab H#, Westhaeusser F#, Ernst A, Yamamura J, Fuhlert P, Zimmermann M, Sauerbeck J, Shenas F, Özden C, Weidmann A, Adam G, Bonn S#, Schramm C#. DeePSC: A Deep Learning Model for Automated Diagnosis of Primary Sclerosing Cholangitis on 2D MR Cholangiopancreatography. Radiol Artif Intell 2023;5:e220160. doi: 10.1148/ryai.220160.
Puelles VG#, Lütgehetmann M#, Lindenmeyer MT#, Sperhake JP#, Wong MN, Allweiss L, Chilla S, Heinemann A, Wanner N, Liu S, Braun F, Lu S, Pfefferle S, Schröder AS, Edler C, Gross O, Glatzel M, Wichmann D, Wiech T, Kluge S, Pueschel K, Aepfelbacher M, Huber TB. Multiorgan and Renal Tropism of SARS-CoV-2. N Engl J Med 2020;383:590-592. doi: 10.1056/NEJMc2011400. Open access.
Braun F, Lütgehetmann M, Pfefferle S, Wong MN, Carsten A, Lindenmeyer MT, Nörz D, Heinrich F, Meißner K, Wichmann D, Kluge S, Gross O, Pueschel K, Schröder AS, Edler C, Aepfelbacher M, Puelles VG, Huber TB. SARS-CoV-2 renal tropism associates with acute kidney injury. Lancet 2020;396:597-598. doi: 10.1016/S0140-6736(20)31759-1. Open access.
Wanner N#, Andrieux G#, Badia-I-Mompel P, Edler C, Pfefferle S, Lindenmeyer MT, Schmidt-Lauber C, Czogalla J, Wong MN, Okabayashi Y, Braun F, Lütgehetmann M, Meister E, Lu S, Noriega MLM, Günther T, Grundhoff A, Fischer N, Bräuninger H, Lindner D, Westermann D, Haas F, Roedl K, Kluge S, Addo MM, Huber S, Lohse AW, Reiser J, Ondruschka B, Sperhake JP, Saez-Rodriguez J, Boerries M, Hayek SS, Aepfelbacher M, Scaturro P#, Puelles VG#, Huber TB#. Molecular consequences of SARS-CoV-2 liver tropism. Nat Metab 2022;4:310-319. doi: 10.1038/s42255-022-00552-6. Open access.
#equally contributing authors